
Case Report | DOI: https://doi.org/10.31579/2578-8868/183
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
2Department of Neurology, Univerity of California, Irvine, California, USA
3China National Clinical Research Center for Neurological Diseases, Beijing, China
4Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences, Beijing, China
*Corresponding Author: Wengui Yu, MD, PhD. Professor of Clinical Neurology Vice Chair for Hospital Affairs, Department of Neurology Director, Comprehensive Stroke & Cerebrovascular Center University of California, Irvine 200 S. Manchester Ave., 206E, Orange, CA 92868 and Xingqu
Citation: Shimeng Liu., Yanfang Liu., Jia Zhang., Wengui Yu., Xingquan Zhao., (2021) Recurrent Hemorrhagic Transformation of Cardioembolic Stroke in an Elderly Patient: A Case Report and Literature Review. J. Neuroscience and Neurological Surgery. 8(5); DOI:10.31579/2578-8868/183
Copyright: © 2021 Wengui Yu and Xingquan Zhao, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 27 April 2021 | Accepted: 03 May 2021 | Published: 10 May 2021
Keywords: hemorrhagic transformation; cardioembolic stroke; antiplatelet therapy; hypertension; diabetes
Proper therapy for secondary stroke prevention is crucial in the management of cardioembolic stroke. Although oral anticoagulants were the superior strategy for patients with atrial fibrillation and stroke per current evidence, many patients with cardioembolic stroke were prescribed with antiplatelet therapy due to concern for the risk of bleeding from anticoagulation therapy. We presented a case of an 84-years-old male patient who had sudden-onset left hemiparesis from cardioembolic stroke. Past medical history was significant for paroxysmal atrial fibrillation, hypertension and uncontrolled diabetes. Severe white matter hyperintensity (WMH) was identified with the brain imaging. The local hospital initiated antiplatelet therapy with Aspirin 100 mg daily for secondary stroke prevention. Subsequently he was found to have recurrent asymptomatic hemorrhagic transformation involving each of the infarctions. The case report highlighted that severe WMH and possible cerebral amyloid angiopathy could be a risk factor of hemorrhagic transformation and antiplatelet therapy should be used prudently in such condition.
Hemorrhagic transformation (HT) of cerebral infarction is a common complication of acute ischemic stroke (AIS) [1, 2]. Symptomatic HT is a risk factor of unfavorable outcomes after AIS [3]. Asymptomatic HT could also be associated with poor outcomes [4]. The frequency of HT was reported to be around 9%. The risk factors of HT include large reperfusion, embolic infarcts, age older than 70 years, renal insufficient, anticoagulant therapy, hypertension, and low low-density lipoprotein (LDL) cholesterol [3, 5-9].
Atrial fibrillation (AF) is a common cardiac arrhythmia. Approximately 20–30% of all ischemic strokes are due to AF [10]. For the patients with an AIS due to AF, it is recommended to initiate oral anticoagulation between 4 and 14 days after the onset of neurological symptoms [11]. However, due to the concern about the risks of HT, many patients with cardioembolic stroke were prescribed with antiplatelet therapy instead of anticoagulation [12].
We report a case of embolic stroke with significant recurrent HTs after receiving Aspirin for secondary stroke prevention. This case report highlights the challenge of secondary stroke prevention for patient at high risk for HT.
An 84-year-old man with a history of paroxysmal AF not on anticoagulation or antiplatelet therapy, chronic hypertension and uncontrolled diabetes was transferred from outside hospital to our comprehensive stroke center for further evaluation and management of AIS and multiple HTs.
Neurological deficits assessments
Stroke severity was determined by using the National Institutes of Health Stroke Scale (NIHSS) [13], a 15-item neurologic evaluation. The NIHSS includes the following domains: level of consciousness, eye movements, integrity of visual fields, facial movements, arm and leg muscle strength, sensation, coordination, language, speech and neglect. Each impairment is scored on an ordinal scale ranging from 0 to 2, 0 to 3, or 0 to 4. Item scores are summed to a total score ranging from 0 to 42 (with higher score indicates more severe the stroke). In the NIHSS scale, a score of < 4 represents a minor stroke, 5 to 15 a moderate stroke, 15 to 20 a moderate-severe stroke, and 21 to 42 a severe stroke.
Clinical outcome assessments
A modified Rankin Score (mRS) was obtained at 3 month to assess the long-term outcome.[14] The mRS is a 6-point, ordinal hierarchical scale that describes “global disability” with a focus on mobility. A mRS score within 0-2 was valued as the functional independent by most studies [15].
Neuroimaging examinations
Head computed tomography (CT) examinations were 64-slice spiral. The brain MRI scans were performed on 3.0‐T scanners, including axial/sagittal T2‐weighted images and T1‐weighted images, axial fluid‐attenuated inversion (FLAIR), axial diffusion weighted imaging (DWI)
with/without Susceptibility-weighted imaging (SWI).
White matter hyperintensities (WMH) burdened were based on FLAIR and T2-weighted images using Fazekas scale [16]. A total score ranging from 0 to 6 was the sum of periventricular and subcortical Fazekas scores.
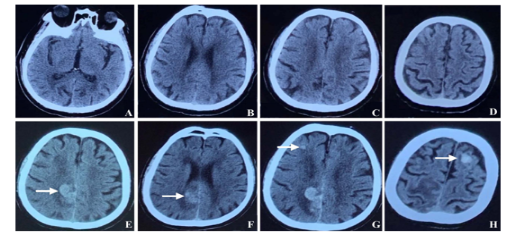
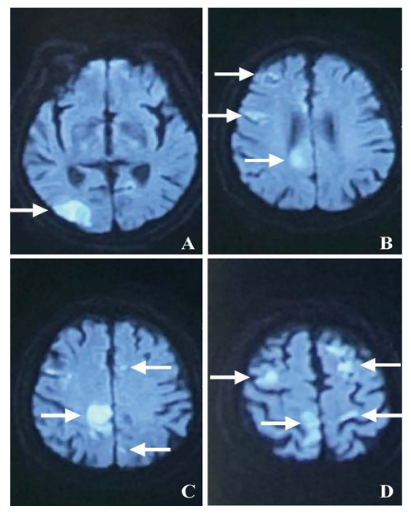
The patient initially presented to the outside hospital with sudden onset left sided numbness, clumsiness and weakness 25 days ago. Non-contrast head CT showed a chronic infarct in the right parietal cortex without evidence of hemorrhage (Figure 1, A-D). Brain MRI showed multiple acute embolic infarcts in both hemispheres (Figure 2, A-D). He was not treated with intravenous thrombolysis, endovascular intervention or anticoagulants. Aspirin 100 mg daily was started for secondary stroke prevention. Follow-up CT scan on day 4 showed HT in the right parietal infarction (Figure 1, E). Aspirin was then discontinued. Repeat CT scan on day 7 showed new HT in the right parietal and right frontal lobe (Figure 1, F & G). CT scan on day 20 day showed a new HT in the left frontal lobe (Figure 1, H).
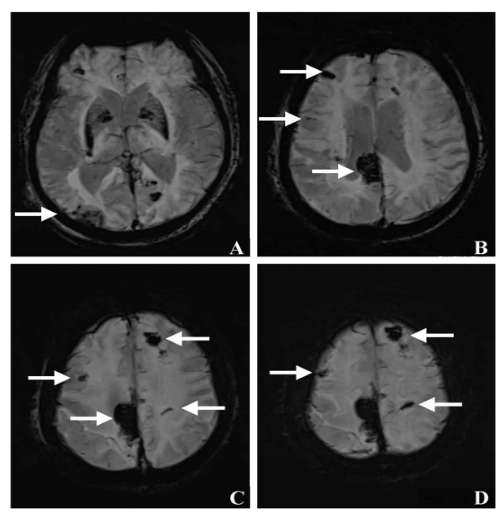
Due to the recurrent multiple HTs, he was transferred to our stroke center for further evaluation at 25 days. At the time of arrival, his blood pressure was 138/105 mmHg, and his pulse rate was 129 bpm. His NIHSS score was 8. Laboratory evaluation did not reveal any evidence of infection. His hemoglobin A1c was 9.7% with fasting blood glucose 13.56 mmol/L. The estimated glomerular filtration (eGFR) was within the normal range. Twelve-lead electrocardiography demonstrated normal sinus rhythm with elongated ST-segment. Transthoracic echocardiography revealed an ejection fraction of 63%, with slightly enlarged left atrial volume (diameter between the anterior and posterior wall: 40 mm; normal range: < 38 mm). No left atrial appendage (LAA) pathology or mitral stenosis was identified. No evidence of systematic or intracranial malignancy were found by Positron Emission Tomography Scan (PET)-CT scan. Brain angiography magnetic resonance angiography (MRA), Transcranial Doppler (TCD) and carotid ultrasonography did not reveal any arterial stenosis or occlusion involving the intracranial or cervical sections. The maximum cerebral lesion diameter of the infarctions ranged 17-34 mm. Of note, the brain MRI showed diffuse deep WMH with a Fazekas Scale score of 3 (Figure 3).

SWI sequence confirmed the diagnosis of HTs. He was discharged with anti-hypertensive and anti-diabetic medications. No anticoagulatant or antiplatelet agent was prescribed due to the recurrent HTs.
His mRS score was 2 at the 3-month follow-up. The brain MRI scan at 3-month follow up showed stable HTs without new infarction or hemorrhage (Figure 4).
The 84-year-old patient had acute embolic stroke. He developed recurrent HTs of the infarctions only after a few days of Aspirin at the local hospital. The AIS was most likely due to cardioembolic source, since the infarctions were distributed in multiple vascular territories. Infectious endocarditis was a major cause of cardioembolic stroke followed by multiple-site HTs [17], but it was ruled out by the negative results of echocardiography and blood tests. Thus, AF was identified as the etiology of the cardioembolism, as the patient had a history of paroxysmal AF for 7 years prior to the symptom onset.
For the patients with an AIS and AF, the American Heart Association (AHA)/American Stroke Association (ASA) recommend initiating oral anticoagulation between 4 and 14 days after the onset of neurological symptoms [11]. Per the AHA/ASA guideline for the secondary stroke prevention [10], male patient with AF and CHA2DS2-VASc score of 2 or greater (6 for the case) should be prescribed with oral anticoagulant. The patterns of AF include paroxysmal (self-limiting and shorter than 1 week), persistent (episodes lasting longer than 7 days) and permanent (AF without any intercurrent sinus rhythm) [18]. Paroxysmal AF was associated with lower risks of yearly ischemic stroke (persistent vs. paroxysmal AF: 3.0 vs. 2.1 %, adjusted HR: 1.44, P= 0.02; permanent vs. paroxysmal AF: 4.2 vs. 2.1%, adjusted HR: 1.83, P < 0.001) [19]. Per the guideline, treatment decision for stroke prevention should not be influenced by AF patterns [18]. But Aspirin was initiated for the case instead of anticoagulant due to concern of HT given the history of chronic hypertension, poorly controlled diabetes and advanced age [11, 18].
Anticoagulant has distinctive pharmacological effects compared with antiplatelet agent: the former prevents the formation of red thrombus, while the latter prevents the formation of white thrombus [12]. The LAA in AF forms the red thrombus, which explains why antiplatelet agents are less effective in preventing stroke from AF.
New direct oral anticoagulants (DOACs) are as efficacious as warfarin for prevention of stroke in AF but are not more likely to cause severe hemorrhage than Aspirin. According to the guideline, for the patients with AIS and HT, initiation or continuation of antiplatelet or anticoagulation therapy was not contradicted [11]. Prior observational studies with limited sample size suggested that antithrombotics can be safely initiated or continued in patients with AIS and HT. In a prospective, open-label study of 60 patients with AF and an AIS with an NIHSS score < 9 or TIA (n=11) who were treated with rivaroxaban within 14 days of onset, HT was present in 25 (42%) patients at baseline. No patients developed symptomatic HT. New asymptomatic HT developed in 3 patients and asymptomatic progression of HT occurred in 5 patients [20]. In another study, Antiplatelet (n=72) treatment after HT was not associated with enlargement of the original HT or development of new HT or neurological deterioration [21].
Besides cardioembolism, the patient has multiple other risk factors of HT, including advanced age, hyperglycemia, hypertension, and hypodensity on head CT [3, 5-9]. The patient has severe WMH, where the underlying pathological changes included hyaline arteriolosclerosis, hyperplastic arteriolosclerosis, or possible cerebral amyloid angiopathy (CAA), added the risks of intracerebral hemorrhage [22]. CAA, cerebrovascular deposition of amyloid-β, was a common finding in the elderly people and a major cause of spontaneous intracerebral hemorrhage (ICH). The key neuroimaging signatures of CAA on clinical MRI include multiple strictly lobar cerebral microbleeds, cortical superficial siderosis, white matter hyperintensities, cortical microinfarcts and MRI-visible perivascular spaces in the centrum semiovale [23]. Thus, CAA was highly suspected as a comorbidity in the case. The impaired function and structure of endothelial cells may increase the risks of HT [24, 25].
Suspected CAA may increase the risks of HT after a cardioembolic stroke, especially in the high-risk patients [26]. The case suggested that WMH could be a warning signal of HT. Antiplatelet was not a better choice than anticoagulants in terms of efficacy or safety for the high-risk patients with AIS and AF.
The observation that some hemorrhagic infarctions develop distal to the site of a persisting occlusion suggests that reperfusion is not always a requirement for HT. Investigators from Japan examined the brains of 14 patients who died from herniation of the brain after cardioembolic stroke with persistent occlusion of the internal carotid-middle arterial axis [27]. The finding of hemorrhagic infarct in 7 of the patients contradicts the concept that reopening a previously occluded vessel is the only pathophysiologic mechanism for the development of hemorrhagic infarct. Analysis of blood pressure after stroke has revealed one or more surges of arterial hypertension or rapid rise of blood pressure in patients with hemorrhagic stroke without a reopening of the occluded artery; it has been speculated that these blood pressure rises might explain hemorrhagic infarction in many cases.
An association between hyperglycemia and hemorrhagic transformation has also been suggested by the observation that occluding the middle cerebral artery of markedly hyperglycemic cats was associated with 5-fold more frequent and 25-fold more extensive hemorrhage into infarcts than in normoglycemic animals [28]. Compared with permanent occlusion, temporary restoration of blood flow after 4 hours caused the most extensive hemorrhage into infarcts. It was concluded that hyperglycemia and restoration of blood flow to ischemic territories were strong risk factors for hemorrhagic infarct conversion. The evidence suggests that the marked tissue energy depletion accompanied by acidosis damages brain vessels, causing leakage of edema fluid and red blood cells [28]. Diffuse HT associated with marked hyperglycemia has been reported in AIS patients [29, 30]. Besides, low high-lipoprotein cholesterol (HDL-c) levels may be connected to the severe WMH and possible CAA and the risk for HTs [31]. The role of aspirin may have effects on HDL-c levels with relevance to disease progression.
Antiplatelet should also be prudently considered for patients with advanced age, cardioembolic stroke, chronic hypertension, poorly controlled diabetes, and suspected CAA.
This work was supported by the National Natural Science Fundation of China under Grant [82001242]; CAMS
Innovation Fund for Medical Sciences under Grant [2019-I2M-5-029]; Beijing Municipal Committee of Science and Technology under Grant [Z201100005620010]; Beijing Tiantan Hospital Traning and Building Program [2-2-2-006-12-04-DR].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
